
Emerging Adults: Bridging the gap between Adolescence and Adulthood
In the early 2000s, developmental psychologist Jeffrey Arnett coined the term “emerging adult” to describe those aged 18-25 [1]. This is a unique period in terms of significant changes in identity development, exploring different roles, and with respect to areas in the brain critical to regulating future-oriented behavior and decision making. Indeed, this period is considered entirely distinct from adolescence and the rest of adulthood.
Nonetheless, in almost all cases, people entering inpatient care at the age of 18 are admitted to a program classified as “adult”. In fact, MHO’s data shows that in 2022-2023, 95% of 18-year-olds and 98% of 19-year-olds that received inpatient care were admitted to adult programs. Furthermore, emerging adults (18 to 25) make up 21% of all adult inpatient admissions, and of note, ages 19, 20, and 21 are the top three most frequent unique ages for adult admissions. Therefore, exploring the needs of emerging adults in inpatient treatment is crucial for tailoring interventions that effectively support their transition into adulthood [2], [3].
Do our emerging adults look the same as all adults?
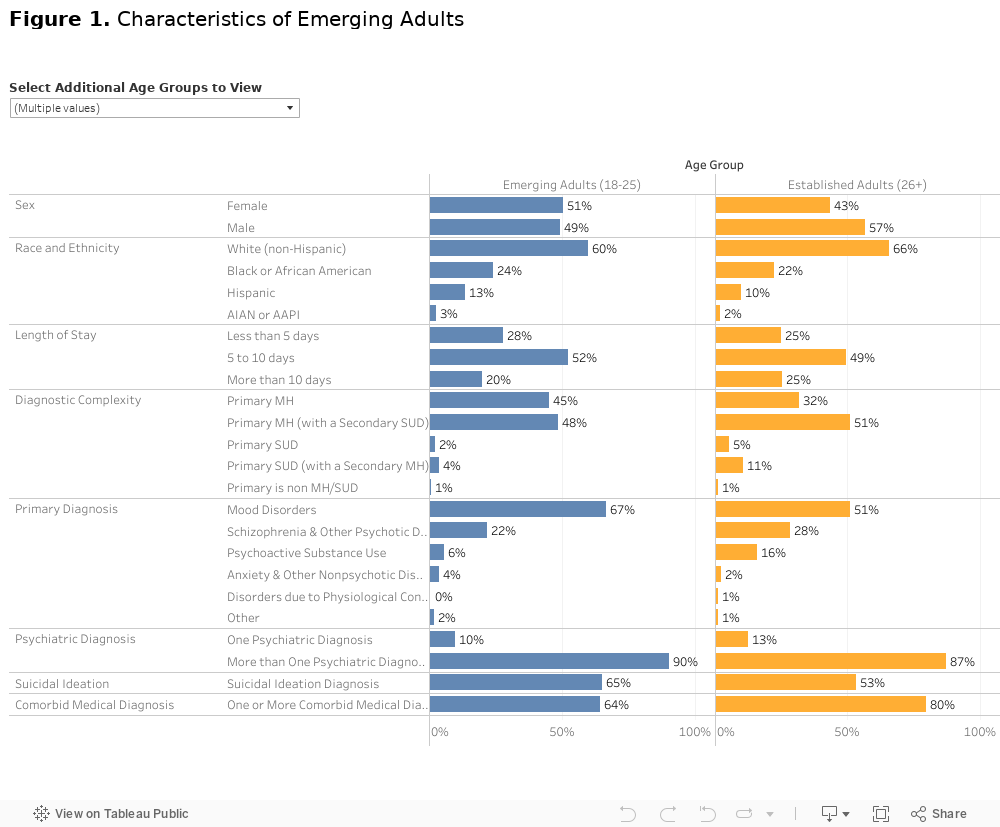
Emerging adults have differences in demographics and clinical presentations compared to older adults. On average they are more often female and less likely to be white compared to older adults. Two-thirds of emerging adults are in care for a mood disorder, compared to only half of the older adult group, and emerging adults have significantly fewer episodes of care for schizophrenia or substance use. Emerging adults are also the only age group where more than half of patients have a recorded diagnosis of suicidal ideation. While over half of all adult inpatients have a dual diagnosis (55.4%), less than half (48.6%) of emerging adults have the same (See Figure 1).
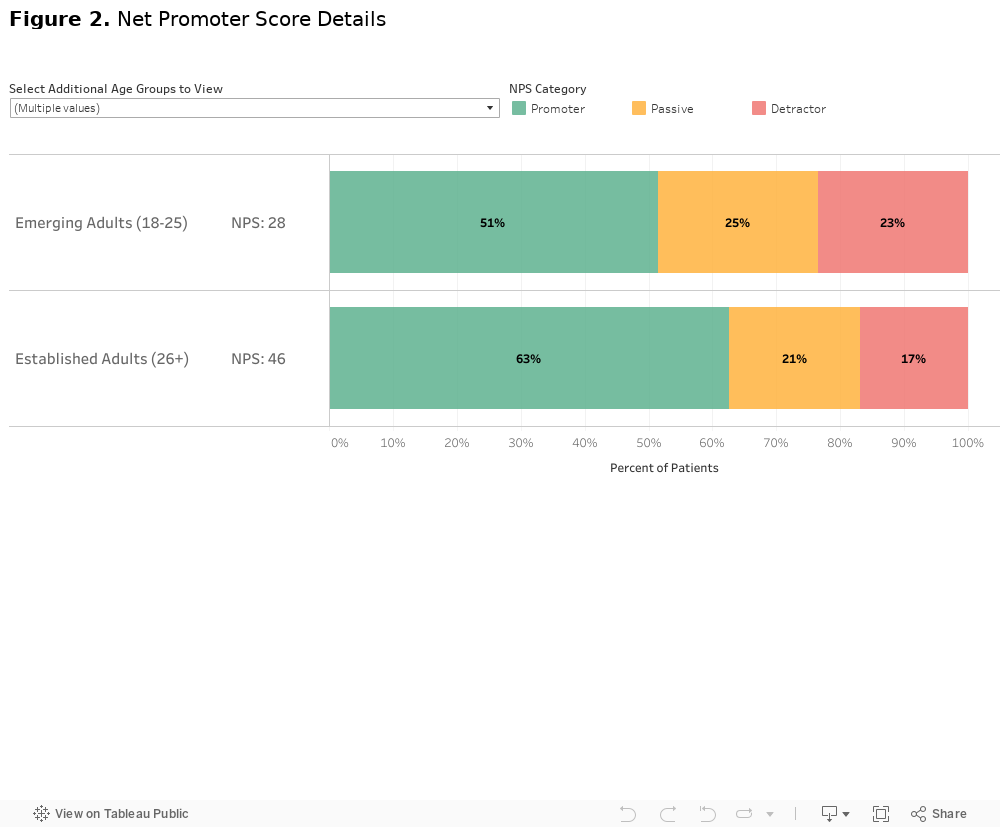
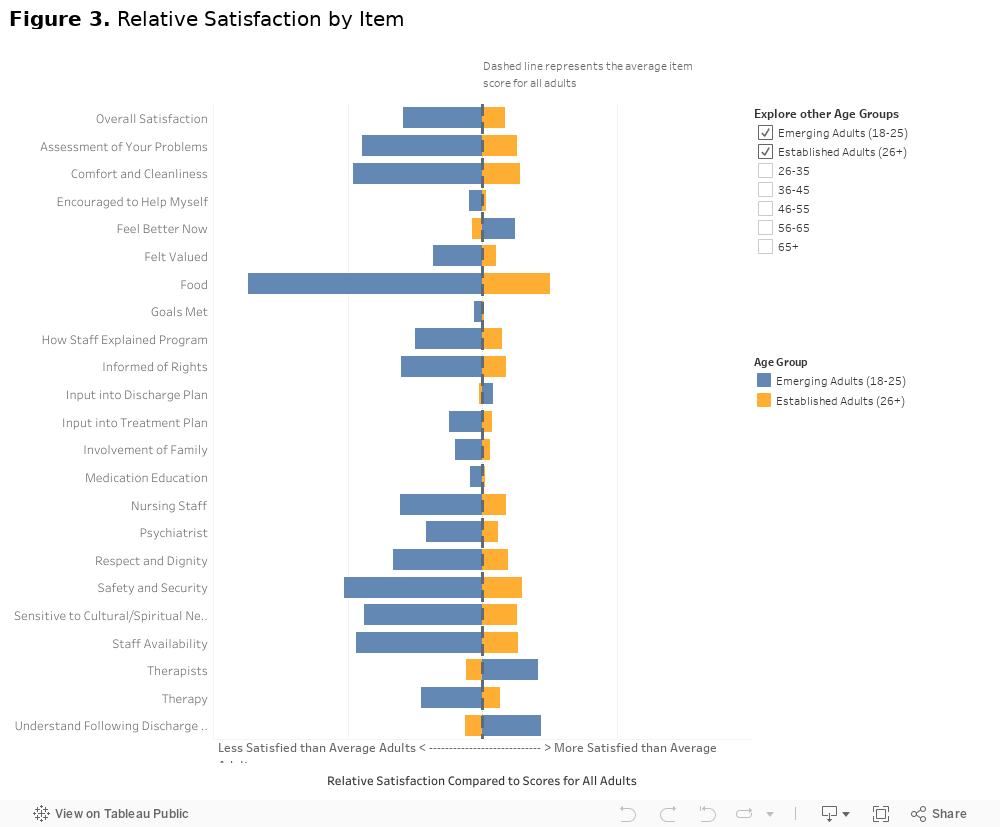
In measures of satisfaction and likelihood to recommend the facility, across the board, emerging adults report less satisfaction with inpatient care. This is the only adult age group where more than 1 in 5 patients are categorized as “detractors”1 of the facility. This group has a Net Promoter Score of 32.34, compared to 45.06 for all adults (See Figure 2). Individual items on the survey can help identify where the biggest gaps in satisfaction are between emerging adults and older adults. Items related to feeling safe, being treated with respect and sensitivity to needs, and food served were all areas of high disparity (See Figure 3). In terms of satisfaction, the common theme driving dissatisfaction is the environment of inpatient care, more so than the care of specific doctors and provided therapies.
What can we do to better serve this age group?
Emerging adults are switching abruptly from a lifetime of health care that has been guided by their parents in collaboration with child and adolescent focused providers to health care in which the patient suddenly interacts directly with providers. In these new interactions, they are without constant input from parents, nor have they developed the skills needed to advocate for themselves [4]. Additionally, they are shifting from care where providers are focused completely on their unique age-appropriate needs to care in which they may feel providers are not experts in their current stage of life, all the while surrounded by other patients who seem to have more “adult” problems [2].
Our findings, similar to other research, show that not only do emerging adults present with a different case mix [5], suggest they value different things while in the treatment setting [4]. Research has demonstrated they are challenged by the idea of restrictive treatment environments and the abrupt disconnection to their usual life (phones, friends, family) that can come with an inpatient admission [6]. So while emerging adults may be in life stages or have preferences that seem incongruous with an inpatient admission, there are ways to improve their experience of inpatient care when it is the best treatment option [3],[7]. These patients will be best supported when their unique needs are met, including care and education focusing on independence, and when surrounded in treatment by patients in a similar stage of life.
Footnotes
- Net Promoter Scores: Net Promoter Score (NPS) is a metric that complements traditional patient satisfaction survey data. The Net Promoter Recommend Question asks patients to respond to “On a scale of 0 – 10, How likely would you be to recommend our facility to a friend or family member?” Patients responding with a score of 9 to 10 are deemed “Promoters”, patients responding 7 or 8 are referred to as “Passives”, and patients responding with a score of 0 to 6 are labeled “Detractors”. The NPS is calculated as the percentage of all promoter responses (9 or 10) minus the percentage of all detractor responses (6 or below). NPS can be as low as -100 or as high as +100, with higher scores being more desirable and indicating a more positive patient experience.
References
[1] Arnett J. J. (2000). Emerging adulthood. A theory of development from the late teens through the twenties. The American psychologist, 55(5), 469–480.
[2] McGorry, P., Bates, T., & Birchwood, M. (2013). Designing youth mental health services for the 21st century: examples from Australia, Ireland and the UK. The British journal of psychiatry. Supplement, 54, s30–s35. https://doi.org/10.1192/bjp.bp.112.119214
[3] O’Donoghue B. (2018). Inpatient care for emerging adults affected by mental health disorders. Early intervention in psychiatry, 12(5), 771–773. https://doi.org/10.1111/eip.12539
[4] Driver, D., Berlacher, M., Harder, S., Oakman, N., Warsi, M., & Chu, E. S. (2022). The Inpatient Experience of Emerging Adults: Transitioning From Pediatric to Adult Care. Journal of patient experience, 9, 23743735221133652. https://doi.org/10.1177/23743735221133652
[5] Twenge, J. M., Cooper, A. B., Joiner, T. E., Duffy, M. E., & Binau, S. G. (2019). Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005-2017. Journal of abnormal psychology, 128(3), 185–199. https://doi.org/10.1037/abn0000410
[6] Haynes, C., Eivors, A., & Crossley, J. (2011). ‘Living in an alternative reality’: adolescents’ experiences of psychiatric inpatient care. Child and adolescent mental health, 16(3), 150–157. https://doi.org/10.1111/j.1475-3588.2011.00598.x
[7] Gaine, G. S., Dubue, J. D., Purdon, S. E., & Abba-Aji, A. (2022). Psychiatric hospital experiences that support and frustrate emerging adults’ psychological needs: A self-determination theory perspective. Early intervention in psychiatry, 16(4), 402–409. https://doi.org/10.1111/eip.13179



