
Medications and Outcomes Data: A Powerful Combination
Practitioners are familiar with the process of clinical trials, arguably the most important step in ensuring safety and effectiveness before a medication can be used in daily clinical practice. However, evaluation of a medication does not end once it is approved and available to patients in ‘the real world’.
Clinical practice, at its core, is rooted in and backed by scientific inquiry. Each time a clinician perceives trends or generalities about Medication A vs. Medication B around anything from patient improvement to side effects to readmissions, they are generating a testable hypothesis. These kinds of hypotheses can be and are tested via formal Phase IV clinical trials, but “real world” data also provide significant opportunity for learnings. In MHO’s case, the most significant opportunity for learning is by combining medications data with standardized outcomes data collected as part of routine clinical practice.
One such high volume case in MHO’s data is within the antidepressant drug class, comparing Escitalopram (Lexapro) against Sertraline (Zoloft) on depression-based clinical outcome tools like the BASIS-32™, PHQ-9, or PHQ-9-A. Here, MHO has more than 5,000 patients in each of these medication-outcomes buckets. Importantly, recent clinical trial research for the effectiveness of these medications on depressive symptoms yields mixed results1, 2. Of course, our interest was piqued in how findings in more typical contexts (e.g., inpatient programs) compared to these results.
Monotherapy Patients
First, inpatients who received only Escitalopram were compared to inpatients who only received Sertraline. In these patients, no other medications could influence the comparison. Demographic and diagnostic information confirm these medications were administered to similar patient populations, ensuring valid clinical comparison (see Demographics Table1 and Diagnoses Table 1).
Demographics Table 1.

Diagnoses Table 1.

Each medication’s discharge and change scores were then compared across outcomes tools, where patients were included only if they had both admission and discharge data for a tool. Although a statistically significant difference emerged on BASIS-32™ change scores, the average difference (0.10 on a 1-4 scale) effect size indicates it is not of clinical relevance (see Figure 1). No other differences were found on discharge or change scores.
Figure 1. Box-and-whisker plots superimposed on jittered raw data. Averages for each cell are represented by dark and dotted black lines. Density of jittered data points indicate the number of patients with scores on that point of the y-axis (higher density = more patients; Interactive Graph)
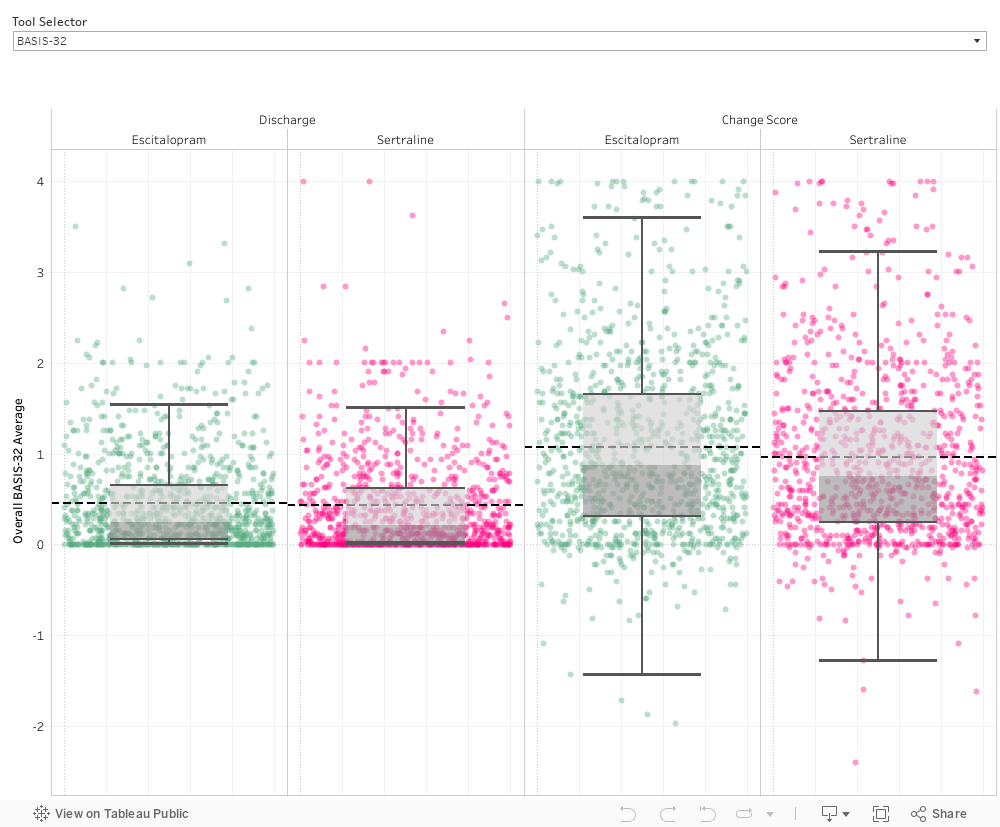
Moreover, each medication had similar percentages of patients with statistically meaningful improvement (SMI) on each tool, further supporting that medications did not differ in clinical outcomes (see SMI Table 1).
SMI Table 1

Polypharmacy Patients
A stronger, even more ‘real-world’ test would compare patients on Escitalopram to patients on Sertraline regardless of other medications, which is the most typical ‘real-world’ scenario (considering 86% of MHO patients are on more than one medication).
To do this, we compared patients who received either medication (but not both) during their inpatient stay. Again, the two medications were used in patients who were similar in demographic and diagnostic characteristics (see Demographics Table 2 and Diagnoses Table 2).
Demographics Table 2.

Diagnoses Table 2.

Each medication’s discharge and change scores were again compared across outcomes tools. Although significant differences emerged on BASIS-32™ discharge and change scores, the average differences (0.03 and 0.08, respectively, on a 0-4 scale) again had an effect size indicating the differences are not of clinical relevance. Similarly, statistically significant differences on PHQ-9 discharge and change scores (0.34 and 0.24, respectively, on a 0-27 scale) were not of clinical relevance (see Figure 2). No differences were found on the PHQ-9-A.
>Figure 2. Box-and-whisker plots superimposed on jittered raw data. Averages for each cell are represented by dark and dotted black lines. Density of jittered data points indicate the number of patients with scores on that point of the y-axis (higher density = more patients; Interactive Graph).
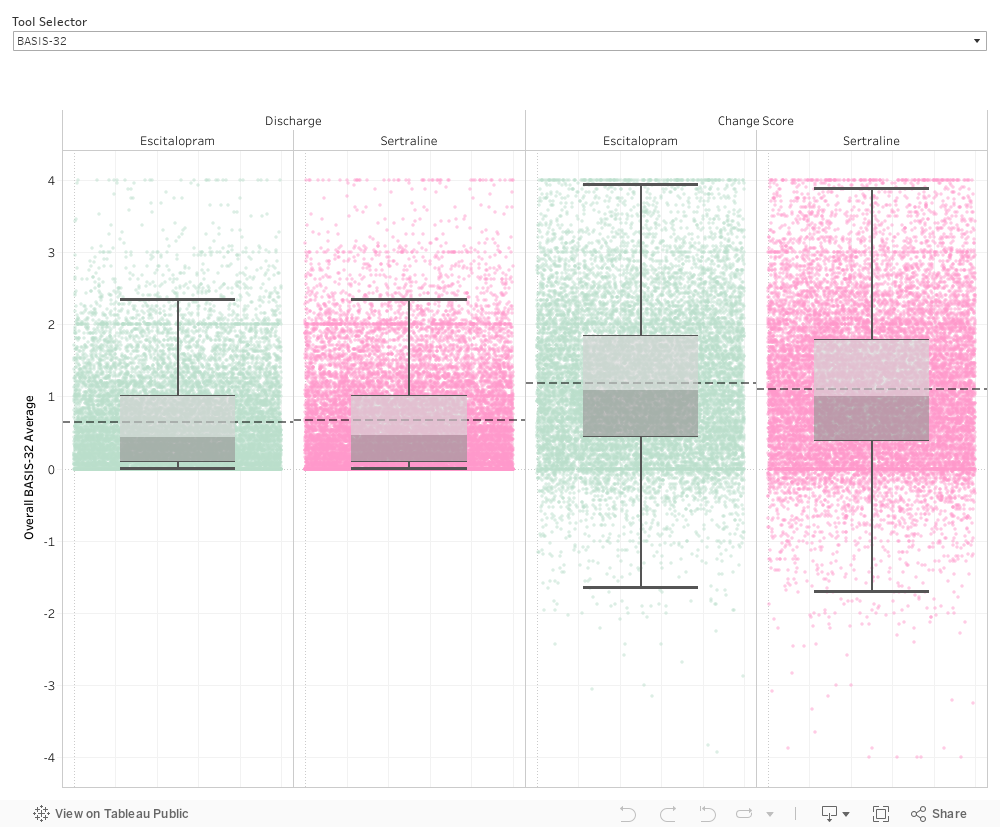
Just as with monotherapy patients, similar percentages of patients showed statistically meaningful improvement (SMI) by medication on each tool (see SMI Table 2).
SMI Table 2.

Conclusion
Both analyses of Escitalopram against Sertraline show patterns most similar to those in prior research described as ‘the real world’3 (i.e., no meaningful difference).
When practitioners know patients have similar outcomes regardless of medication (limitations of this brief analysis notwithstanding), they have additional information to inform their clinical judgment and decision making in the context of other factors. For example, when payers include only certain antidepressants on their approved formularies or when patients have side effects to a specific medication that could compromise adherence.
Analyses such as this are not intended to take the place of high-quality clinical trials. Rather, they supplement and expand our understanding of how to best incorporate medications effectively into both clinical practice and our patients’ everyday lives.
References
- Raza, S., Ahmed, S., Islam, R., Ahmed, M., Ashraf, S., Islam, H., Kiyani, H., Saqib, M., Shah, S. A. R., & Mumtaz, H. (2023). Sertraline versus escitalopram in South Asians with moderate to severe major depressive disorder: (SOUTH-DEP) a double-blind, parallel, randomized controlled trial. Annals of medicine and surgery (2012), 85(10), 4851–4859. https://doi.org/10.1097/MS9.0000000000001185
- Yan, N., Hu, S. (2024). The safety and efficacy of escitalopram and sertraline in post-stroke depression: a randomized controlled trial. BMC Psychiatry,24, 365. https://doi.org/10.1186/s12888-024-05833-w
- Adjei, K., Adunlin, G., Ali, A.A. (2023). Impact of sertraline, fluoxetine, and escitalopram on psychological distress among United States adult outpatients with a major depressive disorder. Healthcare, 11(5), 740.
https://doi.org/10.3390/healthcare11050740


