When patients return to a behavioral health hospital within 30 days, it raises an important question; could this have been anticipated? To better understand what predicts readmission in psychiatric care, we built a statistical model using patient level claims data from Trilliant [1].
Our analysis included 1,425,824 adult patients (18+) across 5,746 facilities in 2024. For each patient, we identified their first psychiatric hospitalization of the year as the index stay and then examined:
-
- Whether a 30‑day psychiatric inpatient readmission occurred
- Whether the patient received step‑down care before readmission (for those who readmitted) or within 30 days (for those who did not readmit)
- Their psychiatric hospitalization history from 2021 to 2024
- Clinical and demographic data
Overall, we found 14.35% experienced readmission within 30 days of their index discharge. Other findings stood out, too.
PRIOR PSYCHIATRIC HOSPITAL UTILIZATION IS THE STRONGEST PREDICTOR
No factor predicted readmission more powerfully than a prior inpatient stay. Compared to patients with no prior admissions in the last three years, patients with prior admissions had greater odds of a 30-day readmission:
-
- 1 prior admission → 1.34× higher odds
- 2–5 prior admissions → nearly 2× higher odds
- 6+ prior admissions → almost 4× higher odds
Prior utilization likely reflects a cluster of underlying vulnerabilities not fully captured in the dataset—chronic illness severity, relapse risk, treatment resistance, medication‑adherence challenges, housing instability, socioeconomic stressors, and outpatient‑access barriers.
Patients with previous inpatient stays are prime candidates for enhanced transitional planning, proactive outreach, and structured follow-up.
INDEX LENGTH OF STAY IS NOT SIMPLE – CONTEXT MATTERS
Although longer hospital stays were associated with lower odds of 30-day readmission, the relationship between length of stay and readmission is not linear – the largest reduction in odds occurs as length of stay becomes more typical rather than very short, while patients with extended stays have a more modest benefit against those with a more typical length of stay. For example, increasing length of stay from 1 day to 7 days was associated with a 13% reduction in the odds of readmission, but increasing length of stay from 7 to 14 days was associated with only a 6-7% reduction in the odds of readmission.
Moreover, length of stay does not operate in isolation. We observed a significant negative interaction between length of stay and discharge pathway, that is:
-
- For patients discharged to step‑down care, the protective effect of a typical to extended length of stay was stronger.
- For patients without step‑down, length of stay had a weaker association with odds of readmission.
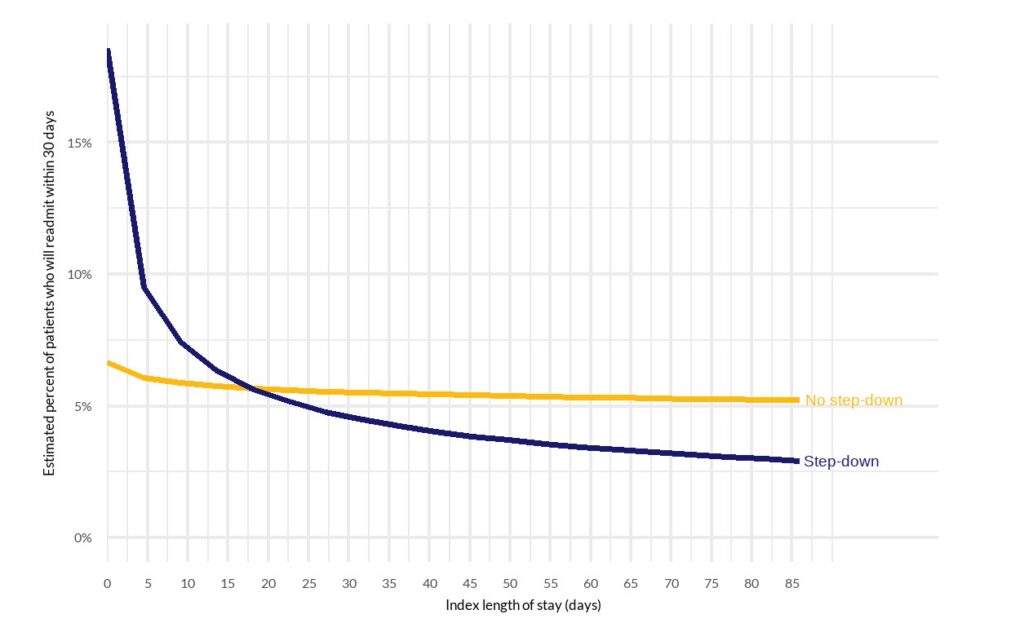
Step-down patients with a very short length of stay have a higher predicted risk of readmission than patients who do not step-down, but as length of stay increases their risk drops more sharply than non step-down patients. With typical and extended lengths of stay, step-down patients can be expected to readmit at a lower rate than those who do not step-down.
Step-down appears most effective when paired with sufficient inpatient stabilization – not as a substitute for it.
Figure 1. For step-down patients only, a typical or longer length of stay significantly reduces the risk of readmission (non-interactive graph)
OTHER FACTORS HAVE A MEANINGFUL BUT SMALLER IMPACT
-
- Diagnosis: Certain diagnostic categories—particularly schizophrenia and substance use disorders—were associated with higher odds of readmission relative to anxiety‑related conditions.
- Clinical severity: Each claim includes a severity indicator – without complications, with complications or comorbidities, or with major complications or comorbidities. Higher severity was meaningfully associated with increased likelihood of return.
- Demographics: Factors such as age and gender contributed modestly to the model’s discrimination compared with diagnosis, severity, prior utilization, and discharge pathway.
WHAT DOES THIS MEAN FOR HOSPITALS?
Readmissions are not random. They cluster among patients with repeated prior utilization and are shaped by the interplay between inpatient stabilization and discharge planning. Three priorities stand out:
1. Identify high‑utilization patients early: Flag patients with prior admissions for enhanced transition planning, assertive follow‑up calls, medication reconciliation, bridge appointments, and community resource linkage.
2. Optimize stabilization before discharge: Adequate length of stay remains protective—especially when step‑down is planned. Avoid using step‑down to “shorten” necessary inpatient stabilization.
3. Align step‑down programming with clinical readiness: Step‑down services work best when they build on, rather than replace, a solid inpatient stabilization period.
REFERENCES
[1] Data source: Trilliant Health