Tracking the Step-Down Journey: Self-Reported Symptom Severity
At MHO, many of the hospitals we work with have a full range of care available, from acute inpatient, through Partial Hospitalization and Intensive Outpatient (PHP/IOP), to traditional outpatient. Patients are placed in different settings depending on their unique symptoms and severity. At different times patients will need to “step-down” from inpatient to PHP or IOP, while other times they may be “stepping up” to inpatient [1], [2]. Step-down care helps maintain inpatient treatment gains while easing patients back into daily life. Understanding what to expect during transition between levels of care can help providers refine discharge plans and address potential roadblocks [3].
Records were examined for step-down patients who, following an inpatient stay, “stepped-down” to PHP or IOP at the same hospital within 10 days of discharge. Almost half (47.7%) of step-down transitions happened next day or with just one day between, while 34.4% have just 2 to 4 days between discharge and admission.
MHO data reveal two phenomena that suggest truly linear improvement is a misconception. We found both a step-down “bounce” in severity between inpatient and PHP/IOP and that longer transitions between the two are associated with a bigger “bounce”.
Step-Down Bounce
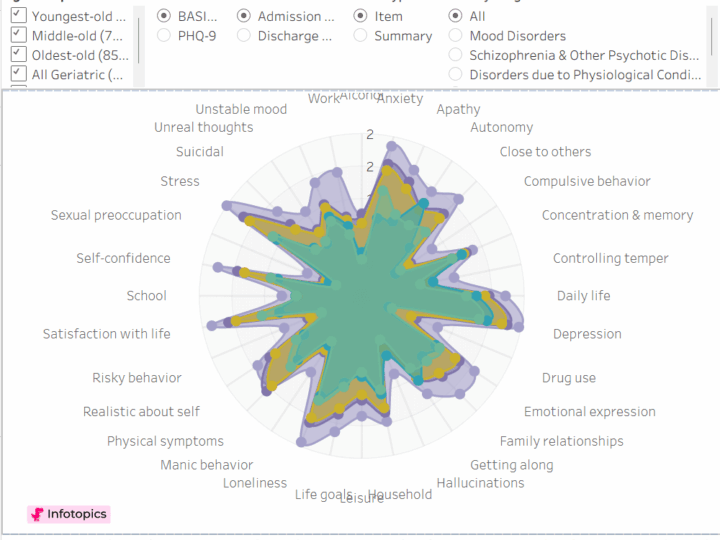
A similar pattern emerged regardless of population (adolescent or adult) and symptoms measured (general functioning or depression). Symptom severity decreased dramatically during inpatient care (~70%). Then, between inpatient discharge and PHP/IOP admission we saw a “bounce” where severity rises and some improvement may seem lost. By PHP/IOP discharge, severity had again fallen, consistent with sustained improvement across the step-down journey.
Figure 1. Patient self-reported symptom severity across continuum of step-down care (Interactive Graph)

Transition Time
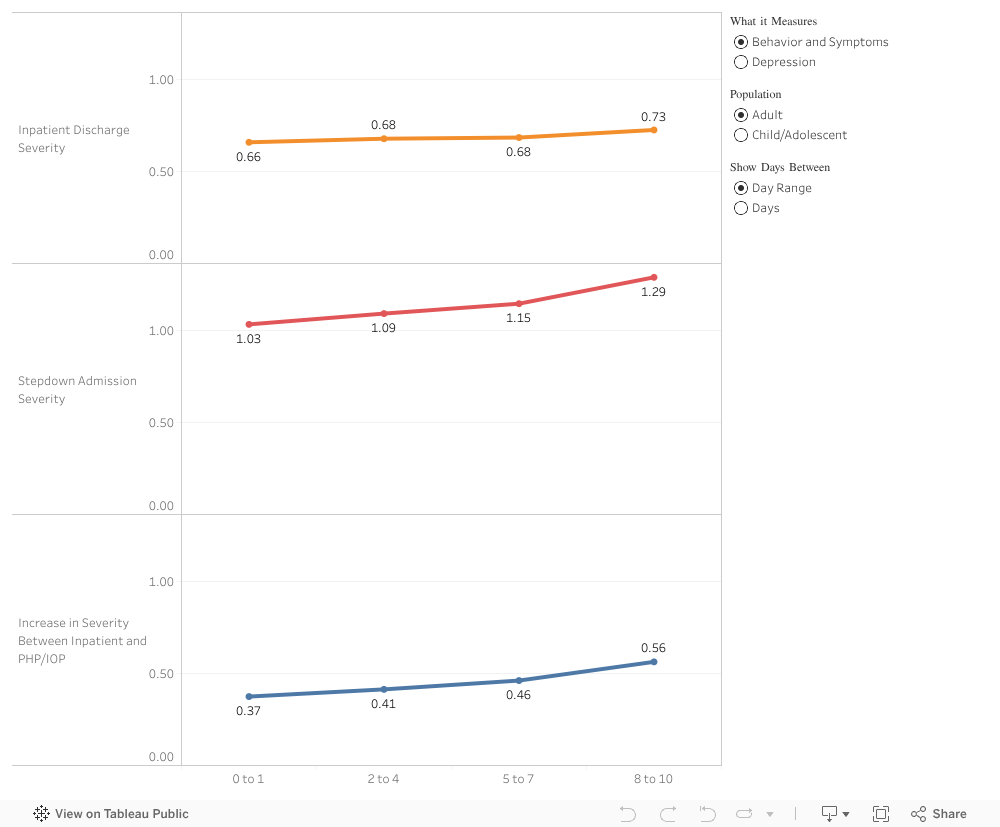
We also find longer waits to begin PHP/IOP result in a larger “bounce”. There are age group and symptom differences, but in general, there are mild correlations between length of the transition period and PHP/IOP admission symptom severity. However, even with next day admission to a step-down program, patients leaving the inpatient environment generally describe greater distress when starting PHP/IOP vs. when they left inpatient care.
Figure 2. Differences in severity changes based on days between inpatient discharge and PHP/IOP admission (Interactive Graph)
Acknowledging the step-down “bounce” in symptom severity between inpatient and PHP/IOP, and the relationship between number of days to transition and size of the bounce, is important. And while these changes may be small, any perceived setback may disrupt the patient’s treatment progress. But the takeaway is ensuring each person who leaves inpatient care understands the importance of step-down care in maintaining gains and, with their care team, has a discharge plan in place for easing transition and addressing roadblocks.
Currently, not all inpatient facilities offer on-site step-down care. One way to facilitate step-down participation is to create partnerships with other agencies to help fill that gap. Some communities may have free-standing PHP/IOP programs that could serve as good step-down options with robust hand-off processes in place. Others might explore their community and consider opening an onsite or satellite PHP/IOP.
Patients may delay entering step-down care because they suddenly feel “better” and do not understand the role of step-down or consequences of longer transitions. Education focused specifically on step-down transitions may be helpful. Patients may also have practical or financial reasons to delay PHP/IOP. Offering treatment programs at different times to accommodate work or easily accessible transportation programs may help.
The best thing behavioral health providers can do to help patients with long-term treatment success is to create integrated systems that allow patients to move along their journey, even though we know it won’t always be a linear path of improvement.
References
[1] Rubenson MP, Gurtovenko K, Simmons SW, Thompson AD. Systematic Review: Patient Outcomes in Transdiagnostic Adolescent Partial Hospitalization Programs. J Am Acad Child Adolesc Psychiatry. 2024;63(2):136-153. doi:10.1016/j.jaac.2023.03.022
[2] Ngo H, Ennals P, Turut S, Geelhoed E, Celenza A, Wolstencroft K. Step-up, step-down mental health care service: evidence from Western Australia’s first – a mixed-method cohort study. BMC Psychiatry. 2020;20(1):214. Published 2020 May 11. doi:10.1186/s12888-020-02609-w
[3] Clarke A, Glick ID. The Crisis in Psychiatric Hospital Care: Changing the Model to Continuous, Integrative Behavioral Health Care. Psychiatr Serv. 2020;71(2):165-169. doi:10.1176/appi.ps.201900259